Most prepper content is written for people who are, medically speaking, fine. They can walk for miles, eat whatever is available, go days without specialized care, and adapt on the fly when plans fall apart.
The world of survival planning generally assumes a baseline level of physical resilience that a significant portion of the population simply does not have. Chronic illness changes the math on everything, and yet the conversation about what preparedness actually looks like for chronically ill people remains frustratingly thin.
According to the CDC, six in ten American adults live with at least one chronic disease, and four in ten live with two or more. For people managing diabetes, autoimmune conditions, dialysis dependency, or active cancer treatment, the supply chain is not a background concern, it is the foreground. Miss an infusion, lose access to refrigeration for insulin, or get stranded three days from your dialysis center during a prolonged grid failure, and the timeline for a health crisis compresses dramatically.
This article is not about making you feel hopeless about your situation, and it is not a denial of how genuinely hard this territory is to plan for. What it is, is a brutally practical look at what realistic preparedness means when your survival window is tied to a fragile medical supply chain.
We will look at what populations in similar historical situations actually did, what your real options are depending on your condition, and what steps you can take right now that could meaningfully extend your window before things become critical. The goal is actionable information, not false comfort.
Understanding What “The Window” Actually Means for Chronic Illness Patients
The first and most important reframe in this kind of planning is shifting from the question of “how do I survive indefinitely?” to “how do I extend my window long enough for systems to partially restore, for aid to arrive, or for alternatives to become available?” That framing is not defeatist. It is actually more functional than the all-or-nothing thinking that causes most people with chronic conditions to avoid this planning entirely.
Different conditions create vastly different window lengths. A well-controlled Type 2 diabetic managing with diet and oral medications has a much longer window than a Type 1 diabetic dependent on rapid-acting insulin analogs that require refrigeration.
Someone on peritoneal dialysis has considerably more flexibility than someone on hemodialysis, who typically needs treatment three times per week to remain stable.
A person on immunosuppressants for an organ transplant faces a different kind of urgency than someone managing rheumatoid arthritis with biologics that, while important, are not immediately life-sustaining in the same way.
Understanding your personal window with clinical honesty is the foundation of everything else. Talk to your physician frankly about what missing one dose looks like, what missing three days of treatment looks like, and what crossing specific thresholds means for your specific physiology.
Many patients have never had this conversation because it feels morbid. Framing it as disaster preparedness planning tends to make it easier for both patient and provider to engage with practically.
What Diabetics Need to Know About Insulin Storage and Supply Rationing
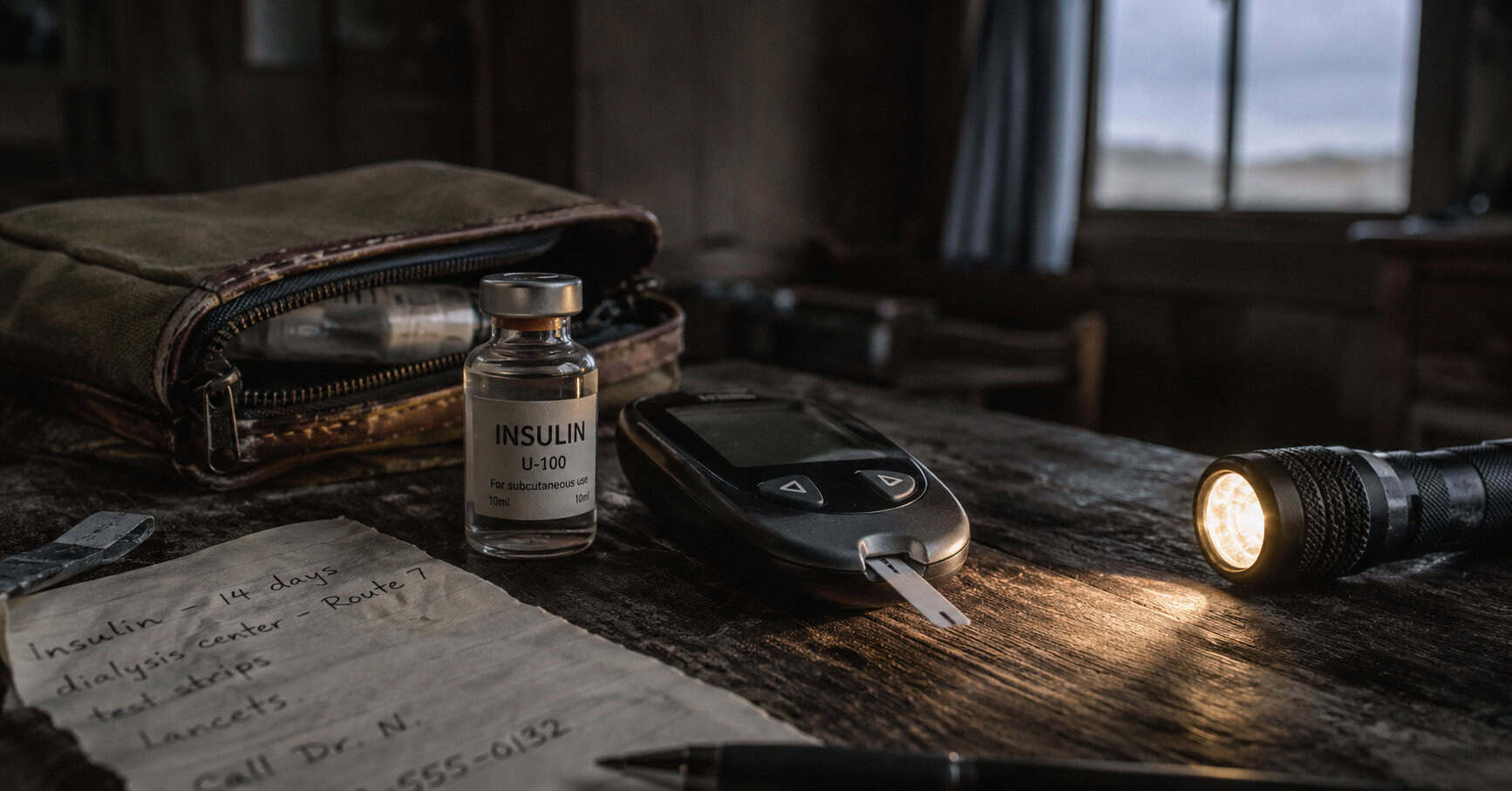
Insulin dependency is one of the most common and most high-stakes chronic illness variables in any collapse scenario. For Type 1 diabetics especially, the math is unforgiving. No insulin means rising blood glucose, and without intervention, that path leads to diabetic ketoacidosis within days. The question of how to extend your insulin supply and keep it viable is worth understanding in real detail.
The good news on storage is somewhat better than most people realize. A Cochrane Collaboration review on insulin thermal stability found that unopened vials of certain human insulin formulations can be stored at temperatures up to 77 degrees Fahrenheit (25 degrees Celsius) for up to six months without clinically relevant loss of potency, and at up to 98.6 degrees Fahrenheit (37 degrees Celsius) for approximately two months. This is meaningful, because it suggests that grid failure alone does not immediately render stockpiled insulin useless, particularly in moderate climates.
The practical implication is that low-tech cooling solutions have real value. Unglazed clay pot coolers, known as zeer pots, work on evaporative cooling principles and can keep contents several degrees cooler than ambient air in dry climates. Wrapping vials in wet cloth and keeping them in the coolest part of a structure, shaded and away from direct light, is meaningful in moderate conditions.
For people who want a reliable portable option to keep temperature-sensitive medications cool during evacuation or short-term grid failure, an insulated insulin cooler travel case with reusable gel packs is a practical starting investment. These are cheap and can save you a lot of headache.
On the rationing side, Type 2 diabetics who are not insulin-dependent have far more flexibility. Extended fasting, strategic carbohydrate restriction, and increased physical activity all influence blood glucose in ways that can reduce medication needs.
Type 1 diabetics cannot eliminate insulin dependency but can reduce their requirements meaningfully through careful diet management and stress reduction. Neither approach eliminates the need for medication, but both extend the operational window significantly.
Autoimmune Conditions and the Challenge of Biologic Medications
People managing autoimmune diseases through biologic medications face a genuinely complex planning problem. Biologics like adalimumab, etanercept, and rituximab are typically delivered by infusion or self-injection and require refrigerated storage. They are expensive, require a functioning pharmaceutical supply chain to manufacture, and in most cases cannot be meaningfully substituted with over-the-counter alternatives.
A peer-reviewed narrative review published in 2024 examined how environmental disasters trigger and exacerbate autoimmune conditions, noting that oxidative stress, immune dysregulation, and disruption of care all compound each other in disaster contexts. The short version of the research is sobering: missing biologic doses tends to result in disease flare, and the physical stress of a disaster scenario is itself an immune trigger. You are dealing with two simultaneous forces pushing in the wrong direction.
The practical planning framework here involves three layers.
First, work with your rheumatologist or specialist to build the largest legally and safely maintainable medication buffer you can. Many insurance plans allow 90-day supplies, and some biologics can be safely stored at room temperature for short periods. Know your specific medication’s storage parameters.
Second, understand what conventional anti-inflammatory medications, particularly corticosteroids, can serve as a bridge in a flare situation when biologics become unavailable. This is not an ideal solution, but it is a real one that your physician can plan for with you.
Third, think seriously about whether your current geographic location makes access to specialized care reasonably achievable in a regional disruption.
For autoimmune patients doing any kind of emergency preparedness, keeping a complete, waterproof copy of your medical records, current medications, dosing schedules, and physician contact information is not optional. First responders who do not know your baseline cannot help you effectively.
Dialysis Dependency: The Hardest Constraint in Chronic Illness Preparedness
Of all the chronic illness scenarios that complicate emergency planning, hemodialysis dependency is among the most constrained. Hemodialysis typically requires three sessions per week, each lasting three to five hours, in a facility with functioning equipment, clean water, and trained staff.
The National Kidney Foundation’s emergency preparedness guidance notes plainly that in a large-scale disaster, patients may not be able to reach a dialysis unit for a period of time and must be ready to manage without treatment for a few days.
A systematic review published in BMC Nephrology examined the effects of natural disasters on dialysis patients in the Americas and found that lack of electricity, clean water, transportation, and the closure of dialysis centers during disasters directly leads to missed sessions, hospitalizations, and emergency department visits. The review’s finding that patient education about emergency renal diets significantly mitigates risk is one of the most actionable takeaways in the disaster medicine literature on this population.
The emergency renal diet is a real clinical tool. Severely restricting potassium intake, which means avoiding bananas, oranges, potatoes, tomatoes, and leafy greens, can significantly slow the dangerous electrolyte shifts that make missed dialysis life-threatening. Limiting phosphorus, found heavily in dairy, nuts, and whole grains, matters as well. Strict fluid restriction reduces the pressure on a non-functioning kidney system.
None of this substitutes for dialysis, but it buys time. Even one or two extra days before a medical crisis develops can be the difference between reaching a functioning facility and not.
Hemodialysis patients should maintain a current list of every dialysis center within a reasonable evacuation radius, not just their primary facility. During Hurricane Katrina, patients who knew the location of alternative facilities and had transportation plans were significantly more likely to continue treatment.
The Kidney Community Emergency Response (KCER) Coalition maintains a locator for dialysis centers that can be checked in advance and should be part of every dialysis patient’s preparedness documentation.
What Chemotherapy Patients Face When the Supply Chain Breaks
Active chemotherapy creates a different kind of vulnerability than maintenance medications. Chemotherapy protocols are often tightly scheduled, and missing treatment cycles affects outcomes in ways that vary enormously by cancer type, stage, and protocol. Some chemotherapy regimens have meaningful tolerance for short delays without significant impact on treatment efficacy while others do not.
This is a conversation that patients need to have with their oncologists specifically, rather than extrapolating from general guidance.
The preparedness planning for chemotherapy patients during a collapse scenario necessarily involves some uncomfortable prioritization. Regional or national disasters that significantly disrupt healthcare infrastructure will affect treatment access. The most realistic planning framework is understanding what a one-week delay means for your protocol, what a two-week delay means, and whether there are treatment facilities outside your immediate area that could serve as alternatives if your primary oncology center becomes inaccessible.
From a practical standpoint, chemotherapy patients face compounding risks during disasters. Compromised immune function from active treatment makes exposure to contaminated water, food, or crowded shelter environments more dangerous. Wound healing is impaired. The physical demands of evacuation may be genuinely beyond current capacity. Planning for chemotherapy patients therefore involves not just medication continuity but a detailed assessment of realistic evacuation options that account for actual physical limitations, and identification of support networks who understand what assistance will actually be needed.
Historical Populations and What Chronic Illness Patients Actually Did
History is not short of examples of chronically ill populations navigating supply chain disruption. The lessons are instructive, though not always comforting.
During the siege of Leningrad from 1941 to 1944, diabetics faced insulin shortages that were essentially unsurvivable for Type 1 patients without access to pre-insulin era management strategies. Those who survived longest typically combined extreme dietary restriction with any available insulin, stretching supplies dramatically. Soviet physicians improvised dose-reduction protocols under extreme duress that, while not optimal, extended survival windows by weeks or months in some cases.
Cuban diabetics during the Special Period following the Soviet collapse in the early 1990s represent a more survivable case study. Cuba’s pharmaceutical supply nearly collapsed, and insulin supplies became severely constrained. The Cuban government’s response included a nationwide shift toward low-glycemic traditional diets, dramatic increases in physical activity through food production labor, and a community health worker system that helped manage patients at the neighborhood level. Type 2 diabetics on insulin were often successfully transitioned to oral medications or diet management during this period, though at significant cost to quality of life and with real health consequences for many.
The 2011 Great East Japan Earthquake provides some of the clearest modern data. Research published afterward found that chronic illness patients, including those with diabetes, hypertension, and respiratory diseases, experienced elevated mortality in the weeks following the disaster, much of it attributable not to direct disaster injury but to medication interruption and care disruption. The populations who fared better were those with some medication stockpile, those near functional secondary care facilities, and those with established community networks.
Building Your Chronic Illness Emergency Medical File
One of the highest-impact, lowest-cost preparedness actions available to any person with a chronic condition is assembling a comprehensive emergency medical file. This sounds mundane, but in disaster scenarios, patients who can hand first responders or emergency physicians a clear, complete picture of their medical status receive dramatically faster and more appropriate care than those who cannot.
Your emergency medical file should contain your full diagnosis list with dates, your current medication list with dosages and frequency, the names and contact information for all your treating physicians and specialists, your pharmacy information, any known drug allergies or adverse reactions, your most recent relevant lab values (A1C for diabetics, kidney function panels for renal patients, etc.), your insurance information, and a brief paragraph describing what a medical emergency specific to your condition looks like and how it should be treated.
This file should exist in at least three forms: a physical copy in a waterproof bag in your go-kit, a digital copy on a USB drive or encrypted cloud storage, and a summary version on a card you carry on your person at all times. A medical alert bracelet or tag that communicates your primary condition to first responders adds another layer of immediate identification that is genuinely lifesaving in situations where you cannot communicate.
Medication Stockpiling: What Is Realistic and How to Approach Your Doctor
The question of how to build a meaningful medication buffer is one that most chronically ill people feel awkward raising with their physicians, often because they worry about being perceived as hoarding or as having unstated intentions. The framing matters here. Presenting the request explicitly as disaster preparedness planning, and referencing guidance from sources like the American Red Cross or FEMA, which recommend maintaining a two-week medication supply as a baseline, tends to be received well by most physicians.
For controlled substances, extended supplies are genuinely harder to obtain and will vary by state, provider, and payer. For non-controlled chronic disease medications, three-month supplies are increasingly standard with mail-order pharmacy programs, and some states have enacted emergency preparedness legislation allowing extended dispensing in declared disaster situations. Know your state’s rules.
Beyond conventional stockpiling, some chronically ill patients in the preparedness community have made the decision to invest in learning about older-generation medications that may be more accessible in a collapsed infrastructure scenario.
For diabetics, this means understanding that older formulations of human insulin, such as NPH and Regular, are available over the counter at certain pharmacies without a prescription in many US states, are less expensive, and are more thermally stable than modern analogs. They require different dosing and carry different risks, but in a genuine supply collapse scenario, they are a known quantity with a decades-long track record.
For monitoring, having a reliable backup blood glucose meter with a substantial supply of test strips and lancets is not optional for any insulin-dependent diabetic planning for disruption. Technology fails, batteries die, and sensors designed for connected systems become useless without supporting infrastructure.
Chronic Illness and Community: Why Isolation Is the Biggest Risk Factor
The research on disaster outcomes for medically vulnerable populations returns consistently to one finding: social isolation is among the strongest predictors of poor outcomes. People who were known to their neighbors, embedded in community networks, and had identified people who would check on them fared significantly better than those who were medically isolated regardless of their condition severity.
For chronically ill individuals doing preparedness planning, this means that community building is not a soft, optional add-on to the harder logistics work. It is core infrastructure. The question of who knows about your medical needs, who has a key to your home, who will notice if you stop responding, and who has the capacity and willingness to assist with evacuation if needed, are all questions with direct mortality implications.
This also extends to identifying others in your community with compatible needs or skills. Nurses, pharmacists, and physicians who live in your neighborhood are potential resources in a sustained collapse. People who manage the same chronic condition you do may have stockpiles, knowledge, or access to medications you lack. Building those relationships before a crisis makes them available during one.
For dialysis patients specifically, the recommendation from the PMC review on disaster preparedness is direct: enroll in your state or local emergency registry for people with special medical needs. Many municipalities maintain these registries to ensure that first responders know about high-priority medical vulnerability in their coverage area. Registration does not guarantee assistance, but it significantly increases the probability of targeted outreach.

The Practical Chronic Illness Go-Kit: What Actually Belongs in It
A standard 72-hour emergency kit is inadequate for most chronically ill people without significant modification. The modification is not complicated, but it requires actually thinking through your specific medical needs rather than buying a generic kit off the shelf.
The foundation is a minimum 14-day supply of all critical medications, stored in clearly labeled containers with dosing instructions included. For insulin, this means vials or pens stored appropriately with a dedicated insulin cooler case and reusable cooling packs. For dialysis patients, it means the emergency renal diet food supply, clear fluid tracking capacity, and documented contact information for every alternative dialysis facility within reasonable reach.
- All prescription medications: minimum 14-day supply with dosing instructions
- Insulin cooling case with gel packs for temperature-sensitive medications
- Blood glucose monitor, extra batteries, minimum 200 test strips, and lancets
- Medical records file in waterproof bag: diagnoses, medications, physician contacts, recent labs
- Medical alert bracelet or card on your person at all times
- Emergency contact list with at least three people who know your medical situation
- Condition-specific emergency diet plan written out and laminated
- Cash in small bills, since pharmacies and medical facilities may not have digital payment
- List of alternative care facilities: dialysis centers, infusion centers, hospitals within 100 miles
- Any necessary medical equipment with battery backup or manual alternatives
The go-kit is not a one-time project. It requires quarterly review to rotate medications before they expire, update medical information as your situation changes, and replace any consumed supplies. Set a calendar reminder. Treat it the same way you treat filling a prescription: non-optional maintenance.
Concluding
Here is what I will say plainly, having spent time with the research and the history: chronic illness does not disqualify someone from meaningful preparedness, but it does require a fundamentally different kind of honesty than the standard prepper conversation allows for.
The honest question is not whether you can achieve total self-sufficiency, because most of us with chronic conditions cannot, and most people without them cannot either, if we are being real about it. The honest question is how many days you can extend, how many options you can open, and how many relationships you can build before something goes wrong.
Every day of medication buffer you build is a day of additional window. Every alternative care facility you have mapped is a route that exists when your primary route closes. Every neighbor who knows about your condition is a person who might notice something is wrong before it becomes irreversible.
The community of chronically ill people in the preparedness world tends to be quietly determined rather than loudly apocalyptic, and that energy feels right to me. You are not planning to thrive without medicine. You are planning to buy yourself enough time for something to become possible. That is a worthy and achievable goal, and it is worth doing the uncomfortable work to pursue it.
This article has been written by James H. Redford MD for Prepper’s Will.
Other Useful Resources:
Drinking Water Survival Myths You Should Know
How to obtain water from the air
The Impacts of Water Scarcity in Major Cities
Knowledge to survive any medical crisis situation during a major disaster